.png)
Why Elastic Tape Is a Game Changer for Phase 2 Lymphoedema Management
- Dec 13, 2023
- 9 min read
Updated: Jan 11, 2025

Manual Therapy gets Stretchy!
The popularity of elastic taping among athletes and health professionals is visible across our sporting screens, and the use of elastic tapes in rehabilitation and scar management is spreading exponentially.
Evidence for the effectiveness of elastic taping as an adjunct in Lymphatic Therapies is also growing, and the most recent Systematic Review (SR) on elastic taping in lymphoedema management supports our collective clinical observations, and confirms that lymph taping is a vital option for people who have trouble applying traditional compression therapies.
This thorough and insightful review also helps guide development of our clinical practice in this evolving therapy.
The review was conducted by by Jaehee Yang RN, RMT, Dr Vodder Therapist (and soon to be MTC Lymph Taping Teacher) in Seoul, as part of her Masters Degree (1).
Are elastic tapes safe and effective in the management of lymphedema?
Jaehee's review aimed to determine whether elastic taping can be used safely and effectively as an alternative or complementary therapy in lymphoedema management.

The short answer is yes, but this review also gives us valuable information that we can apply clinically.
Like all SR which are written as academic exercises, you probably need a higher degree to read and interpret Jaehee's paper, so here are the highlights.
Application methods
As an evolving therapy using an elastic medium, the ways that we can apply the tapes are as varied as the purposes for using the tape. This makes any meta-analysis on the effectiveness of one style of taping over another almost impossible, so a qualitative analysis was used to provide a narrative report on techniques used to apply the tape,
Most of the studies were on breast-cancer related arm lymphoedema with only three studies on taping for neck or face, and one on leg lymphoedema. Tapes were applied as either fan shape tapes, single strips or spirals in any combination, with stretch on the tape ranging between 0% and 25%. Ten of the sixteen studies applied the tape across one or more watersheds, and one used tape only on the unaffected side. The tape in most of the studies was applied from proximal to distal with only two studies using a distal to proximal direction during application.

Only one study compared different taping styles between groups, so there is no clear signal on which taping style, is best. It also can't be concluded whether applying the tape across watersheds offered any added advantage and this needs to be investigated more closely as it is an important, and as yet unanswered, question.
Effectiveness of elastic taping on volume reduction
To determine the effects on volume changes, JaeHee use a meta-analysis to combine the results of eight RCTs on arm lymphoedema which had compared elastic taping and standard compression therapies; multi-layer bandaging (MLB) and compression garments (CG).
The results for each comparison can be seen in the following forest plots. Forest plots show the results of each study as a line which represents the extent of the variation. A square is placed at the mean with the size of the square indicating the size of the effect. The diamond represents the combined results, its relationship to the midline indicates whether it is a statiscitally signficant result, and again, the size of the diamond indicates the effect size.

The six studies included in Graph A show the overall comparison between elastic taping (KT) and any compression, either MLB or CG (Control).
Most of the studies are represented by a wide line with a small square, indicating there was a big variaiton in the between grioup results with only a small difference in mean volume reduction.
The diamond therefore is also small, but is placed entirely to the left of the middline indicating a signficant benefit favouring the elastic taping groups (p < 0.05), but is quite small (mean –7.18). The 95% CI indicaties the variation in the mean results (-12.64, –1.72),
What the forest plot in Graph A does not show is that the MLB groups achieved a great volume reduction than elastic taping alone, so Jaehee looked at some more specific comparisons.
Studies in Graph B compared volume change between MLB with elastic taping (KT), and MLB without the tape (MLB). The forest plot shows a distinct benefit favouring the groups who had elastic tapes added to MLB, and the large diamond indciates the effect size, mean volume reduction (–22.11). It is highly significant (p < 0.001) because of how far to the left of the midline it appears, however the elongated shape also indicates a wider variation in the between group difference in volume reduction (95% CI –32.78, –11.44).
This tells us that while MLB remains the best way to reduce arm oedema, the addition of elastic tapes can significantly improve outcomes, but the exent of the benefit may vary widely.




Graph C shows the volume change between elastic tapes (KT) and compression garments (CG) alone. The very short lines (not much variation in the results), large effect sizes and clustering of the results close to the midline (no significant difference between groups) all tell us that both groups had very similar reductions with no clear advantage to either method.
Which is great news for people with arm lymphoedma who are unable to manage traditional compression garments in the maintenance phase, and definitively tells us that elastic taping is a viable alternative to a compression sleeve if needed.
Effectiveness of elastic taping on shoulder function
Graphs D and E show the comparison between elastic tapes and MLB or CG for range of motion (ROM) of flexion (D) and abduction (E). Although some taped groups showed a greater improvement than un-taped groups, the effect sizes are quite small, and the diamond spans the midline, indicating that the combined results cannot be totally ruled out as having occurred by chance (not statistically significant).




Effectiveness of elastic taping on pain

Previous SR have consistently reported on a reduction in pain when using elastic tapes and Graph F shows the combined result on pain scores in this review. The taped group had a greater reduction in pain than the MLB or CG groups (the diamond appearing to the right of the midline indicates the control group had higher pain scores that the taped groups),
The combined effect size was small, (0.82) but significant (p < 0.001), without much variation (the diamond is narrower) indicating the studies all reported similar results (0.50, 1.15),
Tolerability, adverse effects and quality of life
The primary aim of the review was to determine the effectiveness of elastic taping on symptom relief in lymphoedema, and in all studies taping therapy led to a improvement in quality of life (QOL) with few adverse skin reactions (total incidence 7.7%).
Improvement in QOL will naturally accompany reduction in oedema volume, so the important finding here is that greater reduction in symptoms and improvement in quality of life were experienced in the elastic taping groups, even though MLB usually gave a greater reduction in volume.
Case reports matter

One of the strengths in Jaehee's SR is the inclusion of eight case studies which were all on people who had difficulty applying compression. Reasons for this included presence of an A-V fistula or nerve damage which contraindicated compression, or major discomfort when using MLB or CG.
All eight case studies reported that elastic taping was effective regardless of the site or severity of oedema, and was a suitable alternative where compression was difficult.
One study reported on effective pain relief for a patient with advanced cancer using elastic taping for lower limb lymphoedema, and there were two case studies on people with head and neck lymphoedema who had found compression therapy too uncomfortable, while the tape was both effective and comfortable. Links from the references at the end of the SR will lead you to the original text for these case reports.
Case descriptions offer a more granular view on the effects of lymph taping, but too often SR exclude case studies, thereby losing useful insights which may be clinically valuable.
Summary
The jury is still out on which style of tape is best, but this SR does confirm that whatever the style used, elastic tapes can play an important role in the overall management of lymphoedema.
As noted in the Discussion, results were always better when elastic taping was used in conjunction with compression therapies. This reminds us that our therapies will always have a synergistic effect when applied together, and a great drawback to many SR is the deliberate exclusion of any studies that report on this therapeutic synergy.
This SR confirms for us that taping cannot replace multilayer compression bandaging, but it can improve volume reduction when combined with MLB and will provide similar results to compression garments alone. Elastic tapes also offer greater benefits in pain reduction, treatment comfort and tolerability, and quality of life.
Elastic tapes should be considered as an important adjunct to MLB and a viable option for people who have trouble applying or tolerating traditional compression therapies.
While we wait for the research to catch up....
Our clincal observation on the value of elastic taping to improve symptoms of lymphoedema, to reduce inflammation and acute swelling, and to speed up skin and tissue healing and to reduce scars is still way ahead of the research.
Our New MTC Teacher in Korea
I've had the privilege to work with Jaehee over the last couple of years while she has developed her skills as a Teacher of Lymph Taping, and I'm really proud to welcome her to the MTC Group of Teachers.






Jaehee is also active within her local research community, and during a recent visit to the Department of Rehabilitation Medicine at PNUH (Pusan National University Hospital) she was able to participate in a demonstration on lymphatic mapping using fluoroscopy.



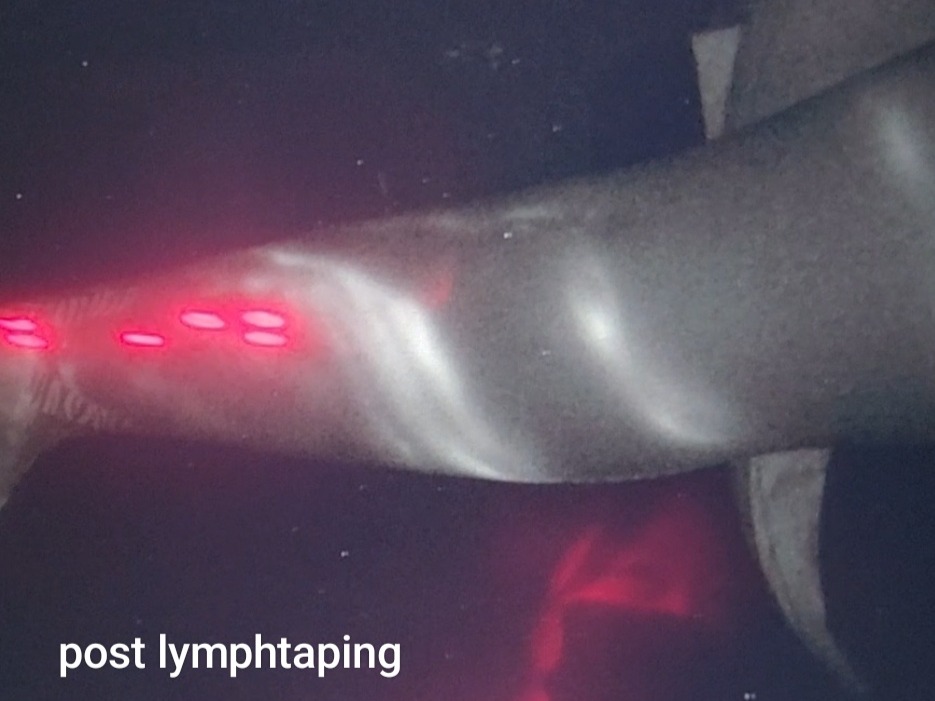
After the ICG tracer had been injected and the superficial lymph pathways began to appear, Jaehee applied some spiral lymph tapes to a healthy arm and the effect of the tape on the ICG tracer was obvious.
The tracer has clearly been drawn into the area under the tape in a distinct pattern which reminds me of the visual effect that occurs when we use lymph tapes over a bruise.
In both cases the lifting and mobilising effect of the tape on the skin draws the macromolecules (ICG tracer or degraded red blood cells) towards the taped area. If you look closely at the bruise image you can see where the dead red blood cells are collecting along the edge of the tape before they are pulled under.




Therapists like Jaehee, and teams like the Rehab Dept at Pusan National University Hospital are helping to moving our understanding on the effect of elastic taping forward, and I'm really excited to see what they will do next year.
Yang J, Lim EJ. A Systematic Review of Kinesiology Taping in Patients With Lymphedema. Physical Therapy Korea 2023;30:288-305. https://doi.org/10.12674/ptk.2023.30.4.288
Abstract
Background: The compression therapy, which is the standard treatment for lymphedema patients, may be difficult to implement and contraindicated to some patients depending on their health condition. Objects: The purpose of this study is to investigate whether kinesiology taping (KT) can be used effectively and safely in the management of lymphedema as an alternative treatment through systematic review and meta-analysis.
Methods: In February 2023, the literature was systematically collected through eight search engines with a combination of terms, ‘lymphedema’ and ‘kinesiology taping.’ We qualitatively analyzed the differences and safety of KT methods, and quantitatively meta-analyzed the effects of volume reduction in edema, range of motion (ROM), and pain improvement using Review Manager ver. 5. 4. To assess the risk of bias in the randomized controlled trial (RCT) studies, Risk of Bias was used.
Results: A total of 616 articles searched and 20 studies were selected, including 12 RCTs and eight case studies. KT intervention could not replace multilayer compression bandage (MLB), but it demonstrated similar or better results compared to compression garment (CG), with reduced pain and improved intervention comfort. Studies reported skin adverse events ranging from 2.5% to 20.68%, with a total adverse event incidence of 7.7%. There was no significant difference in the application method of KT. As a result of the meta-analysis from the 8 RCTs, the KT intervention showed a mean difference (MD) of –7.18 with a 95% confidence interval (CI) [–12.64 to –1.72] in the volume change of lymphedema, while the pain difference was MD 0.82 with CI 95% [0.50 to 1.15], in comparison to the MLB and CG intervention.
Conclusion: KT therapy led to a reduction in edema size, volume, pain, and improved ROM and quality of life. KT may be a viable option for lymphedema patients who have trouble applying traditional compression therapies.



Comments